Acute Kidney Disease (AKD) Models and Efficacy Services
Acute kidney disease, or acute kidney injury (AKI), is characterized by a rapid and often severe decline in kidney function, typically occurring within hours to days. Triggered by diverse factors—severe dehydration, blood loss, sepsis, certain medications like antibiotics and chemotherapy drugs, and impaired renal blood flow—AKI disrupts the kidneys' ability to filter waste, regulate fluid - electrolyte balance, and maintain blood pressure. Symptoms manifest as decreased urine output, swelling, fatigue, nausea, and confusion. Without timely treatment, it can progress to life-threatening complications, including electrolyte disorders, fluid overload, and multi-organ failure. Yet, with prompt diagnosis and proper medical care, many patients can regain normal or near-normal kidney function.
Cisplatin is a widely used chemotherapeutic agent, but due to its significant nephrotoxicity, it is commonly employed to establish AKI animal models. Cisplatin primarily induces renal injury by accumulating in renal tubular cells, causing DNA damage, mitochondrial dysfunction, and cell apoptosis or necrosis. It also reduces renal blood flow, leading to local ischemia and decreased glomerular filtration rate (GFR). This model effectively mimics the pathological features of renal injury observed in patients receiving chemotherapy, including tubular necrosis, inflammatory responses, and oxidative stress, making it a classic experimental tool for studying AKI pathogenesis and evaluating potential nephroprotective therapies.
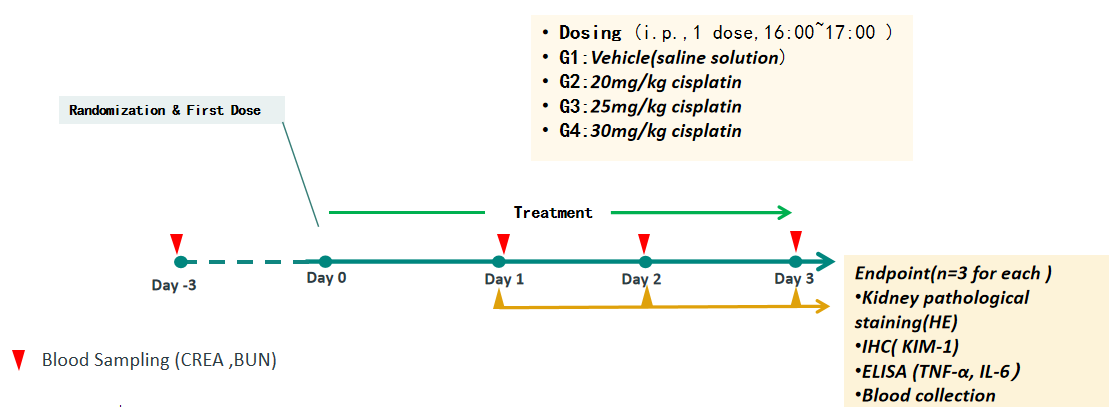
Study Design
Example Data
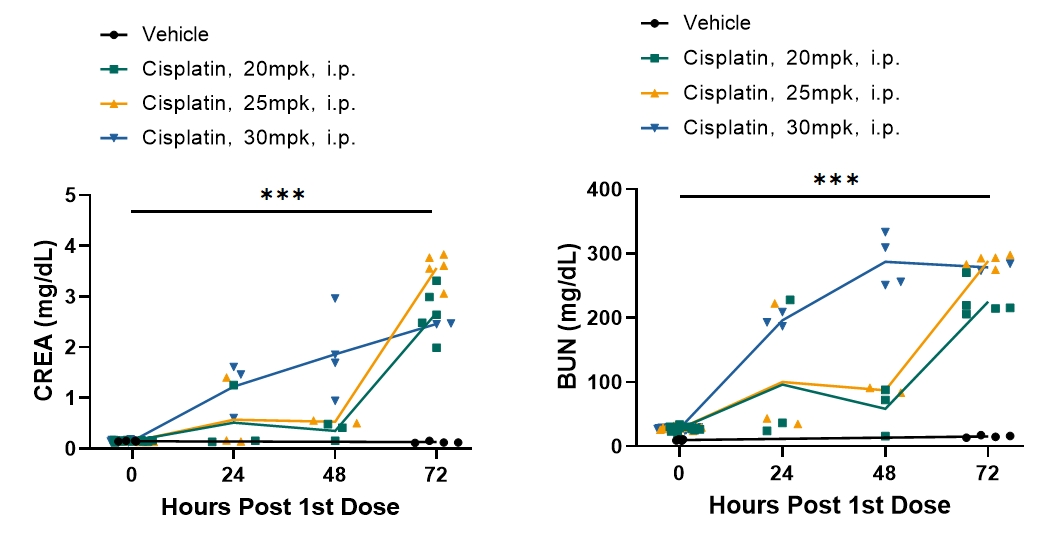
Single cisplatin treatment causes kidney injury in a time-dependent manner
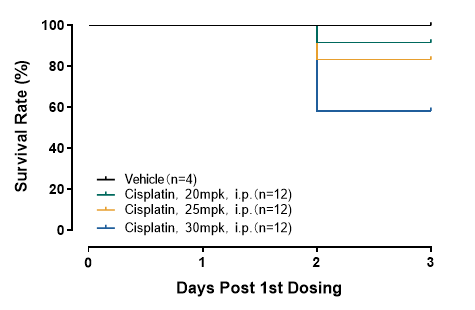
Single cisplatin treatment results in mortality in a dose dependent manner
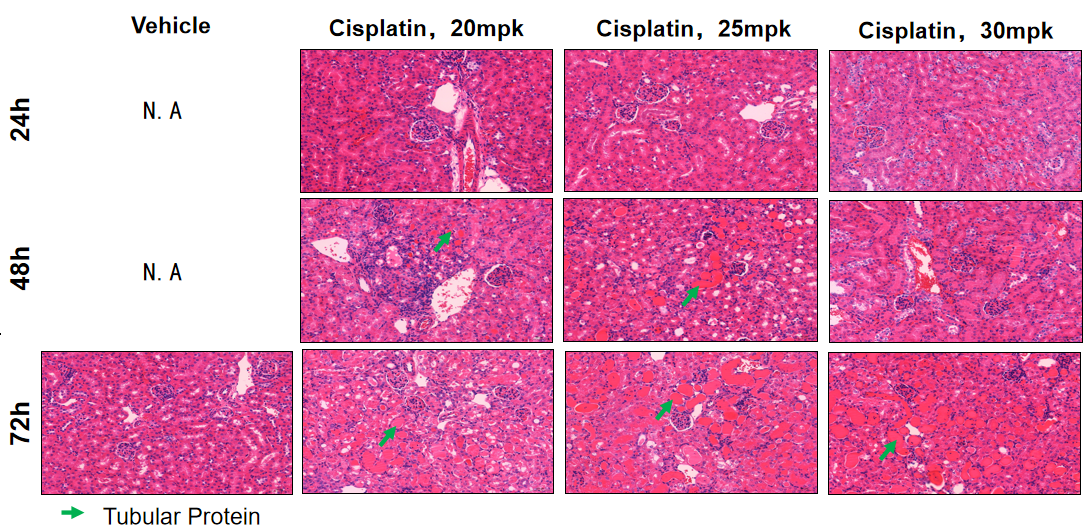
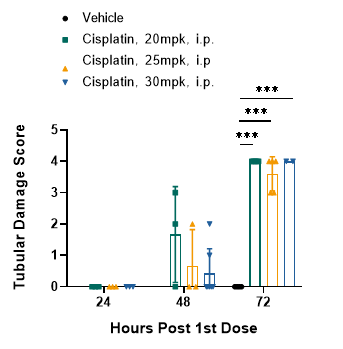
Single cisplatin treatment results in severe tubular damage (tubular protein): Kidney histology (H&E Staining)
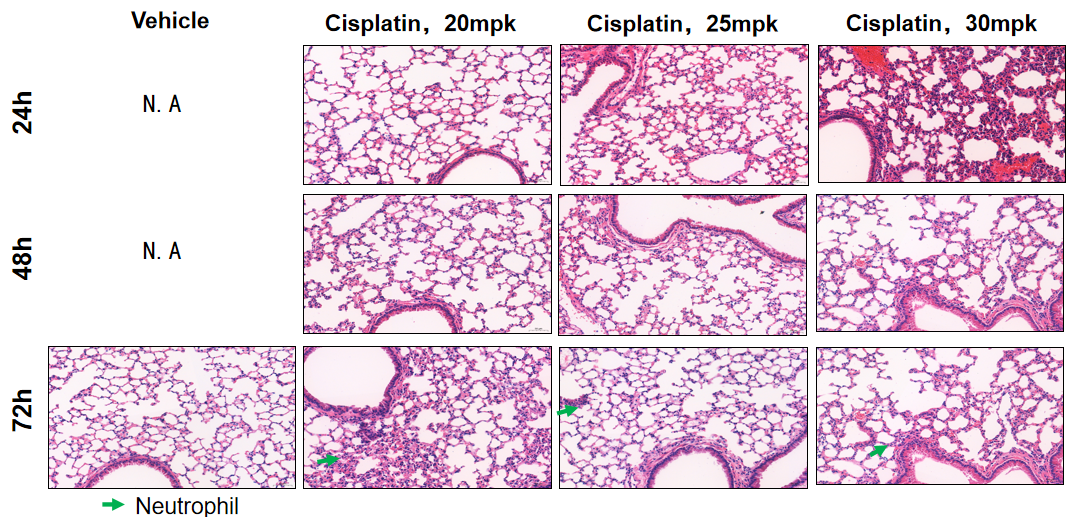
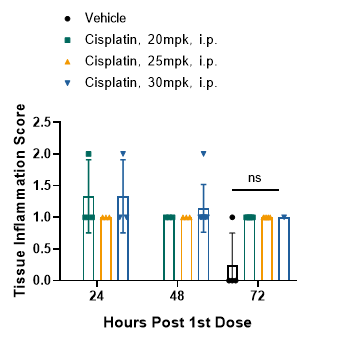
Single cisplatin exposure causes mild inflammation in lung: Lung histology (H&E Staining)