
Advancing In Vivo CAR-T Therapies: Preclinical Evaluation Strategies and Models


In recent years, CAR-T therapy has achieved significant breakthroughs in the treatment of hematological malignancies. However, conventional ex vivo CAR-T approaches require cell isolation, genetic modification, expansion, and reinfusion, resulting in a lengthy, complex, and costly manufacturing process. These limitations have hindered broader clinical development.
To address these challenges, in vivo CAR-T has emerged as a promising next-generation cell therapy approach. This strategy enables the direct induction of CAR expression in target immune cells in vivo via delivery systems, thereby generating cytotoxic CAR effector cells within the body[1]. Compared with traditional approaches, in vivo CAR-T offers advantages in simplified manufacturing, improved accessibility, and enhanced scalability.
In response to growing market demand, and leveraging extensive expertise in innovative animal model development and drug evaluation systems, GemPharmatech now provides comprehensive non-clinical evaluation services for in vivo CAR-T therapeutics.
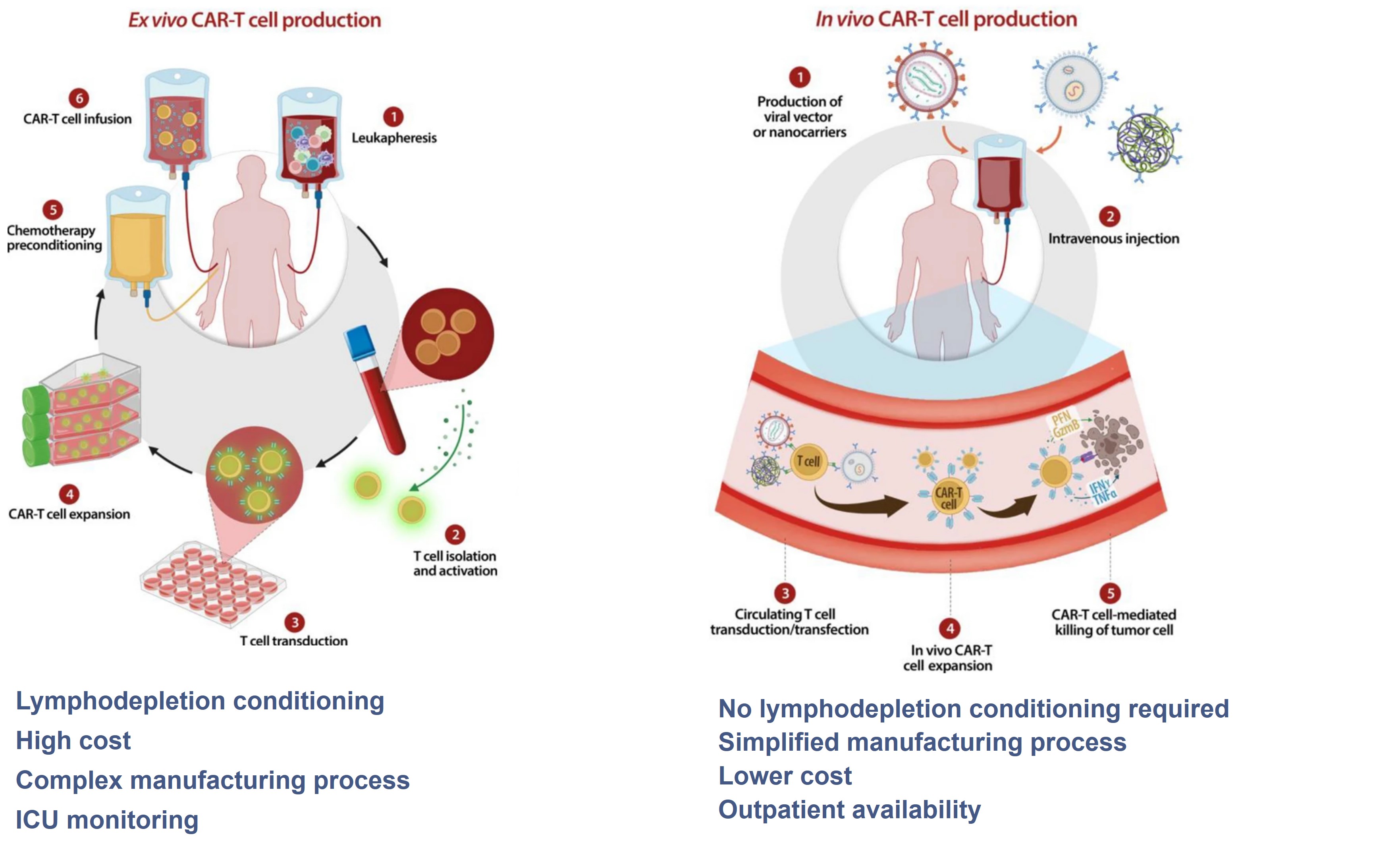
Figure 1. Differences between conventional CAR-T and in vivo CAR-T[1]
1. Design of In Vivo Efficacy Evaluation Systems Based on Delivery Platforms
Currently, in vivo CAR-T delivery strategies can be broadly categorized into:
Viral vectors (e.g., lentivirus, AAV)
Non-viral systems, such as lipid nanoparticles (LNP)
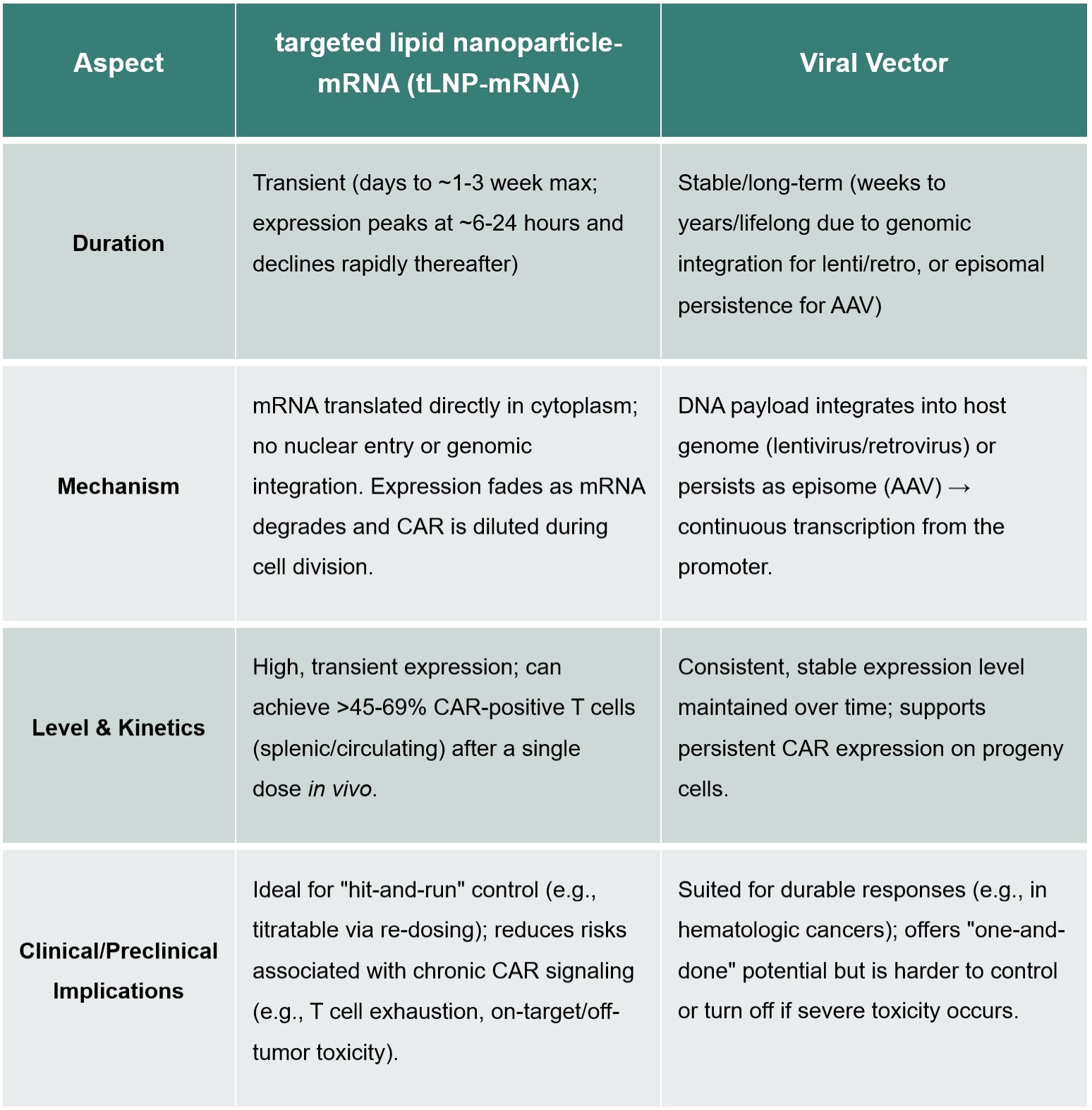
Integrating viral delivery systems (e.g., lentivirus) integrate into the host genome, enabling stable and durable CAR expression. In contrast, LNP systems deliver CAR-encoding mRNA into T cells without genomic integration, resulting in transient expression that typically lasts from several days to about one week.
These differences necessitate distinct experimental design considerations.
Viral Delivery Systems
For viral delivery systems, CAR can be integrated into the genome for persistent expression and proliferates with T cell expansion, so a single dose administration design is usually adopted (Figure 2).
In the case shown in the figure below, NCG-MHC-dKO mice, with MHC class I and II knocked out, can significantly reduce the incidence of graft-versus-host disease (GvHD) after PBMC transplantation and greatly extend the experimental window (≥80 days), making it an ideal model for evaluating in vivo CAR-T therapeutics (Figure 2).
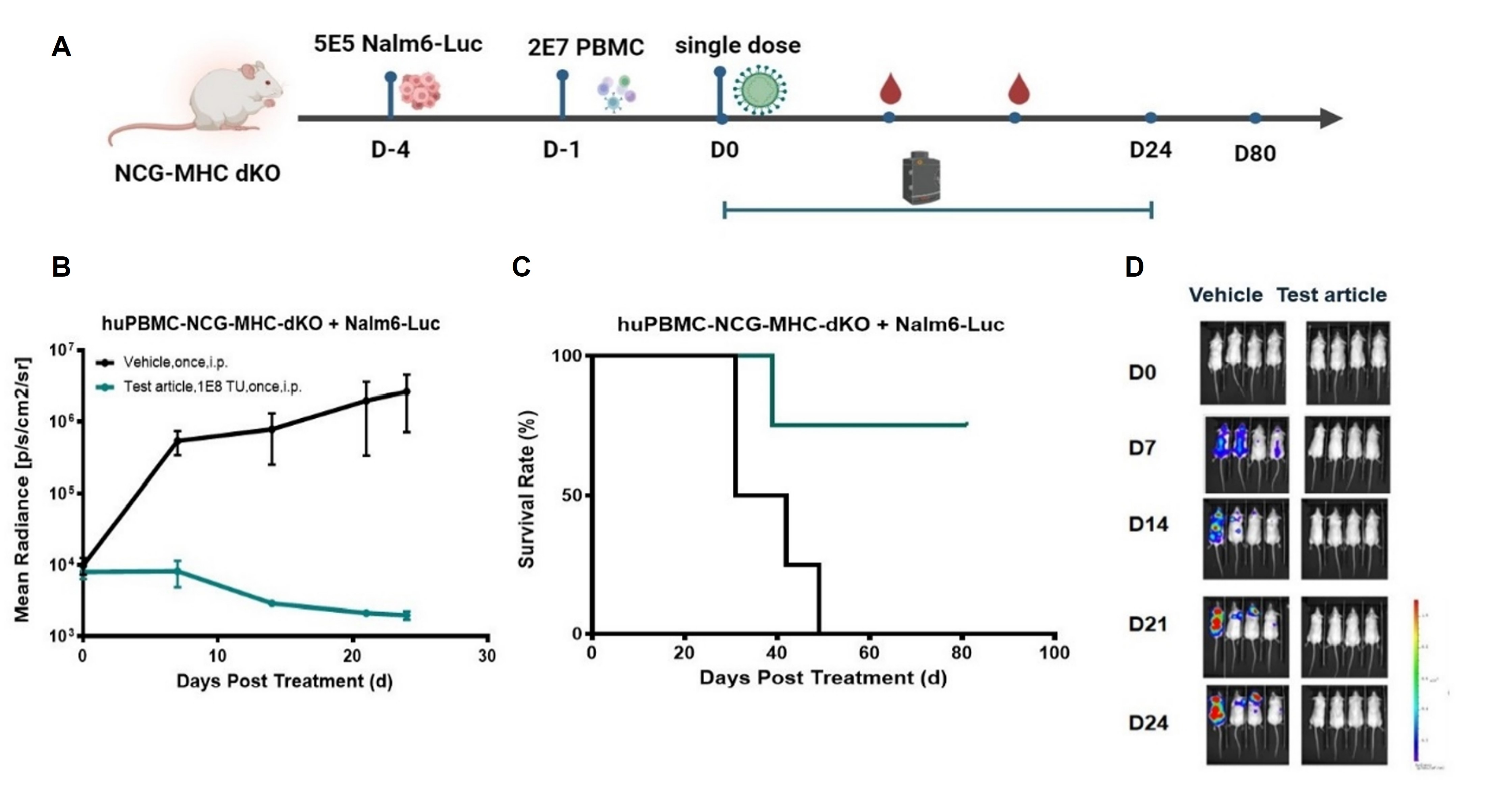
Figure 2. Single-dose efficacy of an integrating viral CAR delivery system in NCG-MHC-dKO mice.
(A) NCG-MHC-dKO mice were engrafted with human PBMC (Day -4) and inoculated with Nalm6-Luc tumor cells (Day -1). A single i.p. dose of test article (1E8 TU) or vehicle was given on Day 0. The test article group showed complete and sustained tumor regression by BLI (B) and 100% survival through Day 80 (C), whereas vehicle controls progressed rapidly and died. Representative images (D) confirm durable tumor control.
LNP Delivery Systems
In the LNP delivery system, LNP delivers CAR‑encoding mRNA into the cytoplasm, which is then translated into protein via transient mRNA expression, relying on the basal level of target cells (usually T cells).
Therefore, multiple administrations are usually required, and there are requirements for the reconstitution level at dosing; administration is generally performed after human CD3+ T cells reach a certain level (Figure 3).
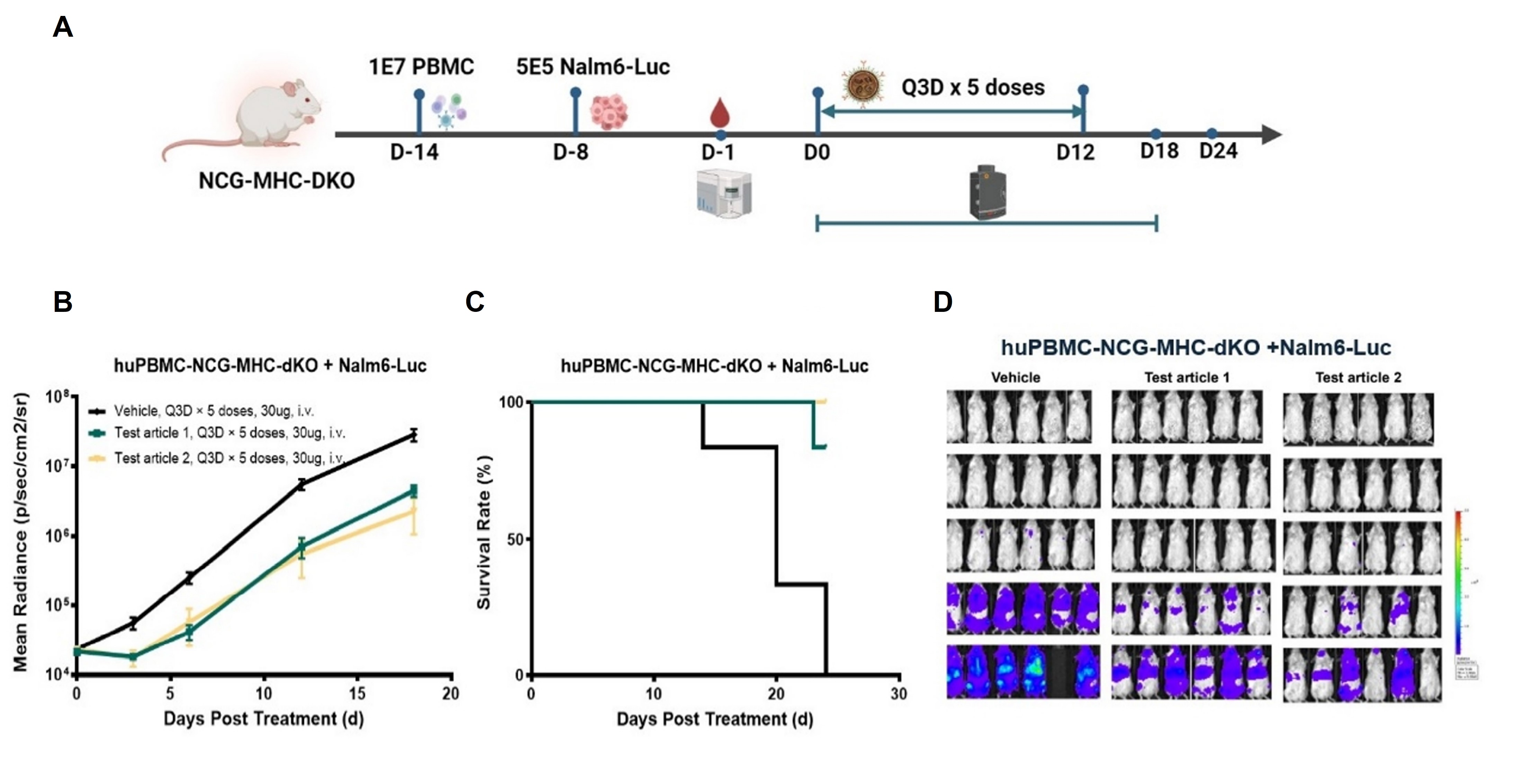
Figure 3. Multi-dose efficacy of LNP-based transient CAR delivery system in NCG-MHC-dKO mice
(A) NCG-MHC-dKO mice were engrafted with human PBMC (Day -14) and inoculated with Nalm6-Luc tumor cells (Day -8). Starting on Day 0, mice received five intravenous doses (Q3D, 30μg each) of vehicle or two LNP-CAR mRNA test articles. Both test articles significantly suppressed tumor growth by BLI (B) and prolonged survival (C) compared to vehicle controls, though transient tumor regrowth between doses was observed due to the non-integrating, transient nature of mRNA expression. The multi-dose regimen (Q3D × 5) compensates for the short CAR expression window (days to one week), enabling sustained anti-tumor efficacy. (D) Representative bioluminescence images from each group visually confirm the tumor burden reduction shown in (B).
GemPharmatech routinely conducts PBMC donor screening in NCG and NCG-MHC-dKO mice. To date, it has established a comprehensive resource bank comprising over 200 PBMC donors and more than 300 CDX models. For widely studied tumor models, such as Nalm-6-luc (CD19⁺), tumor engraftment and donor screening are performed on an ongoing basis to enable rapid response to research and market needs.
2. In Vivo Toxicity and Safety Evaluation for In Vivo CAR-T: huHSC-NCG Model
The huHSC-NCG mouse model is generated by transplanting human CD34⁺ hematopoietic stem cells into sublethally irradiated immunodeficient NCG mice. This model can endogenously reconstitute functional T cells and immature B cells with stable reconstitution levels and long survival period (over 90% survival rate beyond 35 weeks). As a result, it is widely used in B cell depletion, in vivo CAR-T distribution, and long term toxicity and safety evaluation of in vivo CAR-T therapeutics.
This model has been successfully applied in the toxicity and safety evaluation of SYS6055, an in vivo CAR-T therapeutic developed by CSPC Pharmaceutical Group Limited. In addition, the Center for Drug Evaluation (CDE) under the National Medical Products Administration has indicated that PBMC- or HSC-humanized NCG mouse models are appropriate for non-clinical evaluation of in vivo CAR-T therapeutics and can support studies using clinical-grade materials[2].
Given the relatively long model establishment timeline (>12 weeks), GemPharmatech maintains pre-established huHSC-NCG cohorts, significantly reducing study initiation time and accelerating drug development.
Resources and Advantages of GemPharmatech
Leveraging a diverse portfolio of humanized mouse models and extensive non-clinical experience, GemPharmatech provides integrated, one-stop solutions for both in vitro and in vivo evaluation of in vivo CAR-T therapeutics.
Our Advantages:
To accelerate the development of in vivo CAR-T therapeutics, robust and well-designed preclinical evaluation systems are essential. Leveraging advanced humanized mouse models and extensive non-clinical expertise, GemPharmatech is committed to supporting partners in overcoming key translational challenges and advancing innovative therapies toward the clinic.
Interested in learning more? Contact us to discuss how our integrated in vitro and in vivo evaluation platforms can accelerate your in vivo CAR-T development programs.
References
[1] Pinto E, Lione L, Compagnone M, et al. From ex vivo to in vivo chimeric antigen T cells manufacturing: new horizons for CAR T-cell based therapy. J Transl Med, 2025, 23(1): 10.
[2] Zhou Y, Zhang M, Yan LP. Research progress and general non-clinical considerations for in vivo CAR-T. Journal of Regulatory Science and Applications, 2025, 42(6): 409–415.