
Advancing Heart Failure Research: A Comprehensive Guide to Preclinical HFrEF and HFpEF Models



Heart failure (HF) remains a global healthcare crisis, with two distinct phenotypes—Heart Failure with Reduced Ejection Fraction (HFrEF) and Heart Failure with Preserved Ejection Fraction (HFpEF)—posing unique challenges for drug development and translational research. To accelerate breakthroughs, robust preclinical models that recapitulate human disease pathophysiology are essential. Below, we break down a curated panel of validated HFrEF and HFpEF models, designed to empower researchers in selecting the right tool for their studies.
HFrEF Models: Recapitulating Reduced Myocardial Contractility
HFrEF is defined by impaired ventricular ejection fraction, driven by myocardial damage or chronic overload. Our preclinical models replicate these mechanisms to enable mechanistic insights and therapeutic testing:
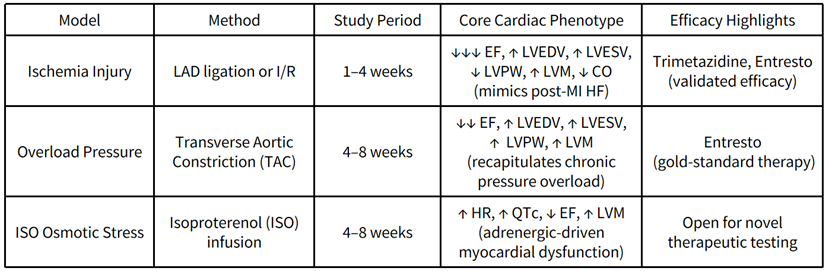
These models are ideal for evaluating drugs targeting myocardial recovery, remodeling, and hemodynamic dysfunction—critical for advancing HFrEF treatments beyond current standards of care.
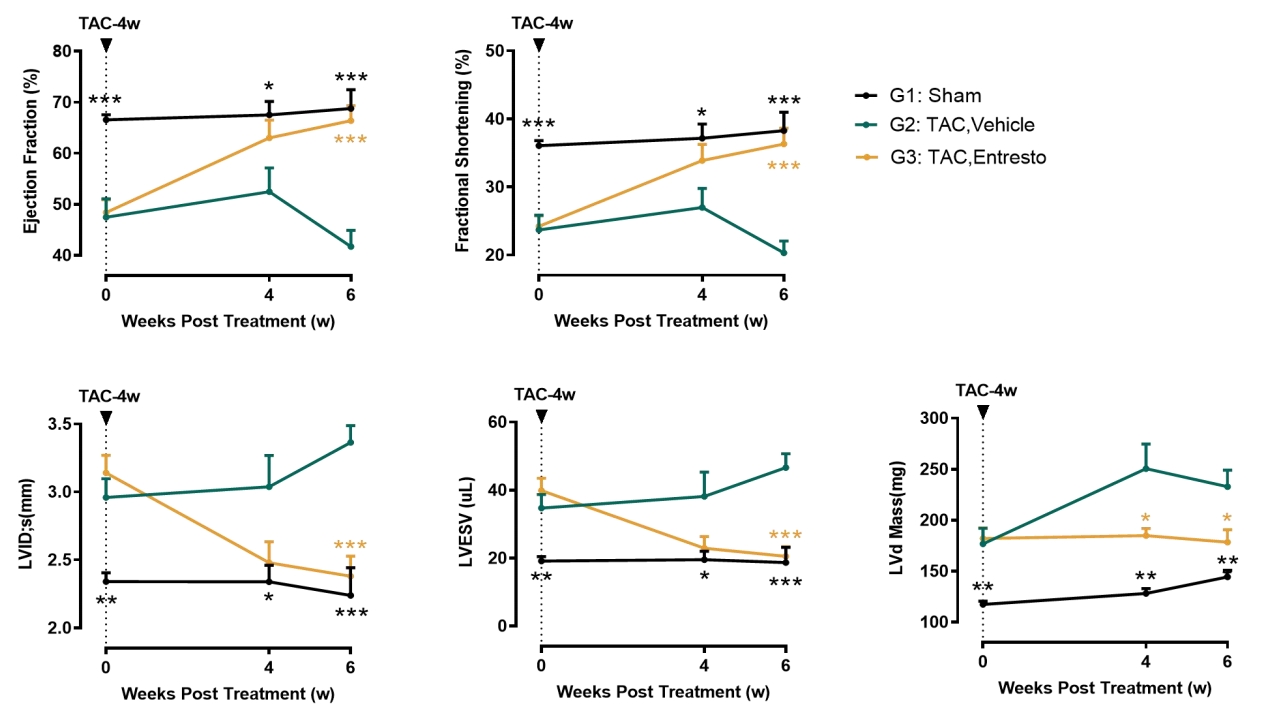
Case Study:
TAC-Induced HFrEF ◄ IND Filing Experience!
This classic HFrEF model is induced by pressure overload. Sacubitril/valsartan shows significant therapeutic benefits in this model.
HFpEF Models: Unlocking the Complexity of Preserved Ejection Fraction
HFpEF accounts for around 50% of HF cases linked to cardiometabolic dysfunction and systemic hypertension.
Our models mirror the multifactorial nature of HFpEF, enabling precision testing of emerging therapies:
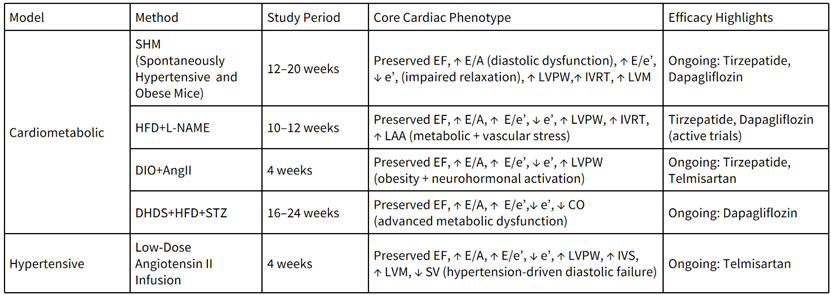
HFpEF’s heterogeneity demands tailored models—our panel spans metabolic and hypertensive etiologies, ensuring researchers can match their hypothesis to a clinically relevant model.
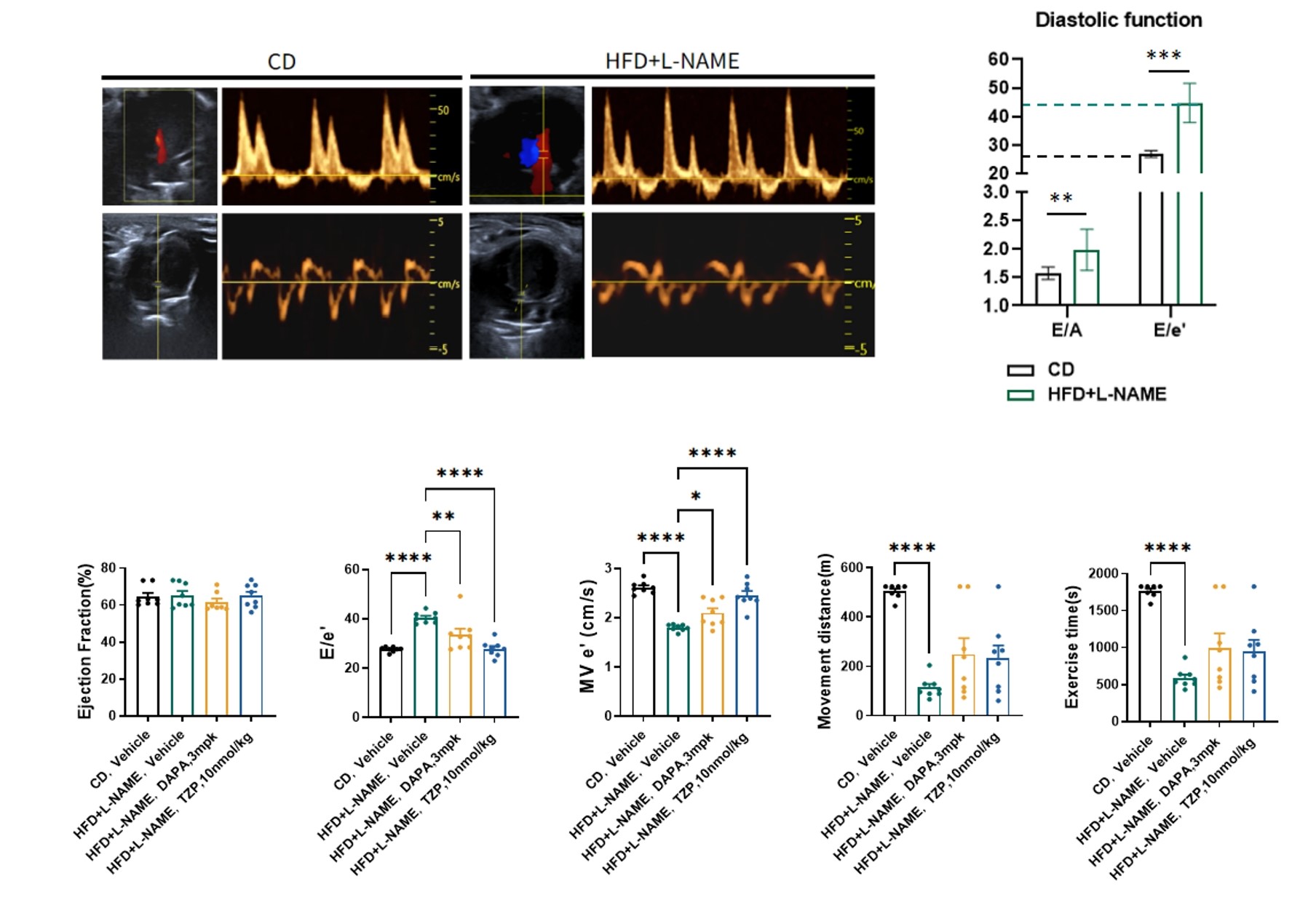
Case Studies:
HFD + L-NAME-Induced HFpEF Model ◄ IND Filing Experience!
This classic HFpEF model effectively simulates microvascular lesions and demonstrates responsiveness to SGLT2i and Incretin drugs.
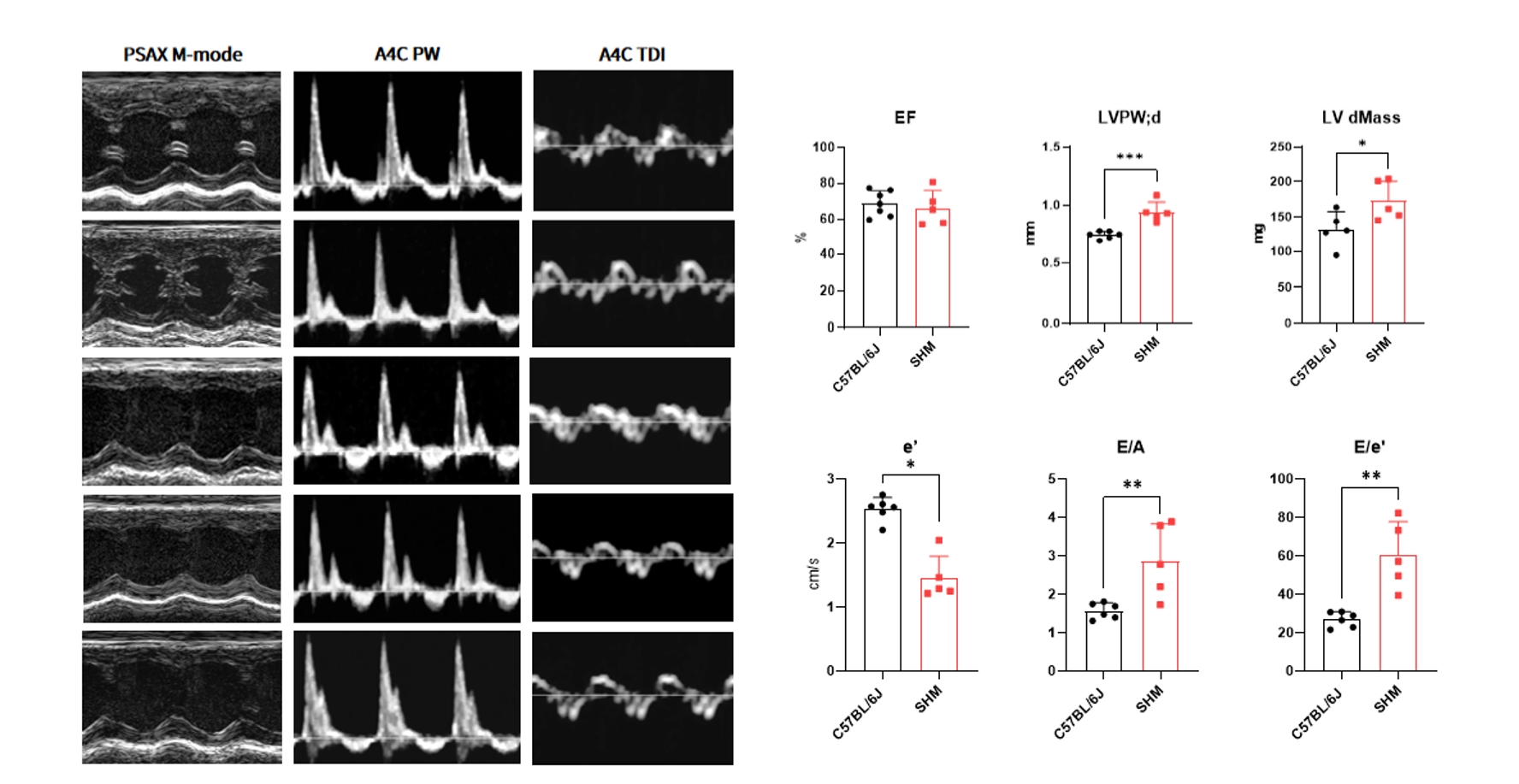
SHM Spontaneous HFpEF Model ◄ Exclusive & Collaborative Model!
This novel HFpEF model spontaneous develop obesity and hypertension, naturally progressing to the HFpEF phenotype at postnatal 20 weeks.
Why These Models Matter for Your Research?
Translational Relevance: Each model is optimized to reflect human HF pathophysiology, de-risking clinical translation.
Therapeutic Flexibility: From validated HFrEF therapies to cutting-edge HFpEF drug candidates (e.g., SGLT2 inhibitors, GLP-1 agonists), these models support phase-appropriate testing.
Mechanistic Depth: Comprehensive phenotypic readouts—including systolic function, diastolic function and cardiac remodeling—enable high-resolution, granular analysis of disease progression and the mechanistic action of therapeutic agents.
Ready to Advance Your Heart Failure Research?
Explore our full model catalog to select the ideal preclinical tool, or collaborate with our team to customize models for your unique scientific goals. Together, we can accelerate the next generation of HF therapies.
Heart Disease | ||
Heart failure with reduced ejection fraction (HFrEF) | STEMI | Left coronary artery ligation (LAD) |
Ischemia reperfusion (Myocardial ischemia/reperfusion injury) | ||
Pressure-overload | Transverse aortic constriction (TAC) (High Demand!!) | |
Chronic (βR activation) | ISO osmotic pump | |
Heart failure with preserved ejection fraction (HFpEF) | Cardiometabolic | HFD+L-NAME (High Demand!!) |
HFD+Ang II | ||
Diabetic heart disease susceptible mice (Exclusive!!) | ||
Spontaneously hypertensive and obese mice (Exclusive!!) | ||
Hypertensive | AngII osmotic pump | |
Cardiomyopathy | Hypertrophic | Mybpc3 KO |
Myh6 R404Q (High Demand!!) | ||
Coronary Heart Disease | ||
Coronary heart disease | ApoE-/-, SR-BIΔCT (Simulate Plaque Rupture in Clinical Atherosclerosis in Mice) | |
Comorbidity | ||
CKM syndrome | BKS-db, AAV-mRenin (Exclusive!!) | |